|
| Solution Notes | |||||
| Title: | Are You Really Sure the Problem is That Serious? | ||||
|
The following are answers to the questions specifically asked in the PBL: 1. Compartment syndrome of the leg involving the lateral compartment only (anterior and posterior compartments were not involved), probably resulting from a tear of the peroneus longus muscle. 2. The lateral compartment of the leg contains the following anatomical structures:
The superficial fibular nerve innervates the fibularis longus and fibularis brevis muscles.
The fibular nerve is part of the lumbar plexus, originating from the sciatic nerve, exiting the spinal cord by spinal nerves L4 to S3. The sciatic nerve passes inferiorly posterior to the femur and deep to the long head of the biceps femoris. As it approaches the popliteal fossa the sciatic nerve divides into the common fibular and the tibial nerve. The common fibular nerve leaves the popilteal fossa by crossing the lateral head of the gastrocnemius and becomes cuteneas in proximity to the head of the fibula. It penetrates the posterior intermuscular septum to enter the lateral compartment of the leg. Shortly after entering the lateral compartment the common fibular nerve divides to form the superficial and deep fibular nerves. The superficial fibular nerve travels inferiorly in the lateral compartment of the leg, at first between the fibula and the fibularis longus muscle, and then between the fibularis longus and fibularis brevis muscles. The deep fibular nerve passes anteriorly, around the head of the fibula, deep to the fibularis longus muscle, and immediately enters the anterior compartment of the leg. It then passes deep to the extensor digitorum longus muscle, moves anteriorly to lie anterior to the interosseous membrane alongside the anterior tibial artery. The nerve eventually comes to lie between the extensor hallicus longus and tibialis anterior muscles. At the ankle the nerve emerges to lie between the tendons of the extensor hallicus longus and tibialis anterior muscles. 3. The vascular supply of the anterior and lateral compartments of the leg are supplied by the anterior tibial artery and supplemented by branches of the posterior tibial and fibular arteries. The anterior tibial artery starts in the posterior compartment as a terminal branch of the popliteal artery. It enters the anterior compartment by passing through a gap in the superior aspect of the interosseous membrane. It passes inferiorly, lying against the anterior surfice of the interosseous membrane and medial to the anterior tibial nerve. Superior to the ankle the anterior tibial nerve passes posterior to the anterior tibial nerve, coming to lie lateral to the nerve as it passes deep to the extensor retinaculum at the ankle. The vessel is now termed the dorsalis pedis artery as it passes the ankle joint. The anterior tibial artery gives off several branches as it moves inferiorly:
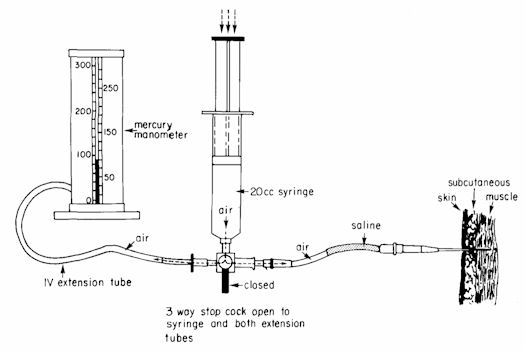
The posterior tibial artery starts in the posterior compartment, at the inferior border of the politeus muscle, as a terminal branch of the popliteal artery. It passes inferiorly with the tibial nerve on the posterior surface of the tibialis posterior muscle. As it reaches the plantar surface of the foot it divides into the medial and lateral plantar branches. Slightly inferior to its origin, the posterior tibial artery gives off it largest branch, the fibular (peroneal) artery. The fibular artery provides most of the vascular supply to the posterior and lateral compartments of the leg. The fibular artery passes laterally across the surface of the bitialis posterior muscle to lie between the interosseous membrane and the fibula. As it passes inferiorly it gives off muscular branches to supply muscles in the anterior and lateral compartments. Superior to the ankle the fibular artery gives off a perforating branch through the interosseous membrane to reach the lateral aspect of the leg and dorsum of the foot. Several methods are used for measuring compartment pressure (Van Ryn, DE. Compartment Syndrome. In: Roberts, JR, Hedges JR, eds. Clinical procedures in emergency medicine. Philadelphia: WB Saunders; 1085). Typically the methodology of Whitesides et al. (1975) is utilized, which involves inserting an 18 guage needle into the compartment and after 1 ml. of normal saline is injected the needle is connected to a pressure monitoring system. The pressure monitoring system is typically composed of a mercury manometer, 20cc syringe, and intravenous extension tubuing partially filled with saline all connected via an open three-way stopcock. (Figure 1). Measurements via this methodology are reportedly accurate to ±3 mmHg of actual compartment pressure. Normal pressures are typically less than 30 mmHg (usually 10–20 mmHg). Pressure in this individual’s lateral comparment was found to be 63 mmHg, while the pressure in the anterior compartment was 105 mmHg.
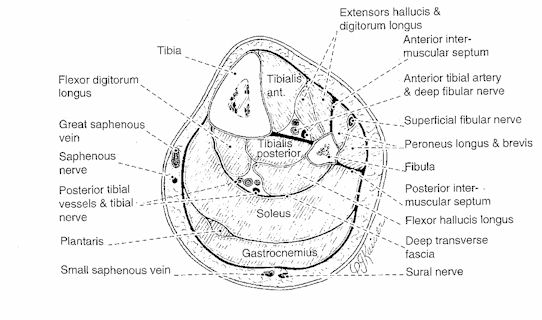
5. "Fasciotomy" is defined in Stedman’s Medical Dictionary as “an incision through a fascia used in the treatment of certain disorders and injuries when marked swelling is present or anticipated which could compromise blood flow.” 6. Briefly, the tibia and fibula, crural interosseous membrane, and septa in the leg create four major compartments: an anterior compartment, a lateral compartment, and superficial and deep posterior compartments. The anterior compartment contains muscles that dorsiflex the ankle, extend the toes, and invert/evert the ankle. The muscles of the lateral compartment evert and plantar flex the ankle. The superficial muscles of the posterior compartment plantar flex the ankle, while those of the deep posterior compartment plantar flex the ankle in addition to their specific actions on the joints of the foot and the toes. (see Figure 2)
|
|||||